More comfortable online than out partying, post-Millennials are safer, physically, than adolescents have ever been. But they’re on the brink of a mental-health crisis.
One day last summer, around noon, I called Athena, a 13-year-old who lives in Houston, Texas. She answered her phone—she’s had an iPhone since she was 11—sounding as if she’d just woken up. We chatted about her favorite songs and TV shows, and I asked her what she likes to do with her friends. “We go to the mall,” she said. “Do your parents drop you off?,” I asked, recalling my own middle-school days, in the 1980s, when I’d enjoy a few parent-free hours shopping with my friends. “No—I go with my family,” she replied. “We’ll go with my mom and brothers and walk a little behind them. I just have to tell my mom where we’re going. I have to check in every hour or every 30 minutes.”
Those mall trips are infrequent—about once a month. More often, Athena and her friends spend time together on their phones, unchaperoned. Unlike the teens of my generation, who might have spent an evening tying up the family landline with gossip, they talk on Snapchat, the smartphone app that allows users to send pictures and videos that quickly disappear. They make sure to keep up their Snapstreaks, which show how many days in a row they have Snapchatted with each other. Sometimes they save screenshots of particularly ridiculous pictures of friends. “It’s good blackmail,” Athena said. (Because she’s a minor, I’m not using her real name.) She told me she’d spent most of the summer hanging out alone in her room with her phone. That’s just the way her generation is, she said. “We didn’t have a choice to know any life without iPads or iPhones. I think we like our phones more than we like actual people.”
I’ve been researching generational differences for 25 years, starting when I was a 22-year-old doctoral student in psychology. Typically, the characteristics that come to define a generation appear gradually, and along a continuum. Beliefs and behaviors that were already rising simply continue to do so. Millennials, for instance, are a highly individualistic generation, but individualism had been increasing since the Baby Boomers turned on, tuned in, and dropped out. I had grown accustomed to line graphs of trends that looked like modest hills and valleys. Then I began studying Athena’s generation.
Around 2012, I noticed abrupt shifts in teen behaviors and emotional states. The gentle slopes of the line graphs became steep mountains and sheer cliffs, and many of the distinctive characteristics of the Millennial generation began to disappear. In all my analyses of generational data—some reaching back to the 1930s—I had never seen anything like it.
At first I presumed these might be blips, but the trends persisted, across several years and a series of national surveys. The changes weren’t just in degree, but in kind. The biggest difference between the Millennials and their predecessors was in how they viewed the world; teens today differ from the Millennials not just in their views but in how they spend their time. The experiences they have every day are radically different from those of the generation that came of age just a few years before them.
What happened in 2012 to cause such dramatic shifts in behavior? It was after the Great Recession, which officially lasted from 2007 to 2009 and had a starker effect on Millennials trying to find a place in a sputtering economy. But it was exactly the moment when the proportion of Americans who owned a smartphone surpassed 50 percent.
The more I pored over yearly surveys of teen attitudes and behaviors, and the more I talked with young people like Athena, the clearer it became that theirs is a generation shaped by the smartphone and by the concomitant rise of social media. I call them iGen. Born between 1995 and 2012, members of this generation are growing up with smartphones, have an Instagram account before they start high school, and do not remember a time before the internet. The Millennials grew up with the web as well, but it wasn’t ever-present in their lives, at hand at all times, day and night. iGen’s oldest members were early adolescents when the iPhone was introduced, in 2007, and high-school students when the iPad entered the scene, in 2010. A 2017 survey of more than 5,000 American teens found that three out of four owned an iPhone.
The advent of the smartphone and its cousin the tablet was followed quickly by hand-wringing about the deleterious effects of “screen time.” But the impact of these devices has not been fully appreciated, and goes far beyond the usual concerns about curtailed attention spans. The arrival of the smartphone has radically changed every aspect of teenagers’ lives, from the nature of their social interactions to their mental health. These changes have affected young people in every corner of the nation and in every type of household. The trends appear among teens poor and rich; of every ethnic background; in cities, suburbs, and small towns. Where there are cell towers, there are teens living their lives on their smartphone.
To those of us who fondly recall a more analog adolescence, this may seem foreign and troubling. The aim of generational study, however, is not to succumb to nostalgia for the way things used to be; it’s to understand how they are now. Some generational changes are positive, some are negative, and many are both. More comfortable in their bedrooms than in a car or at a party, today’s teens are physically safer than teens have ever been. They’re markedly less likely to get into a car accident and, having less of a taste for alcohol than their predecessors, are less susceptible to drinking’s attendant ills.
Psychologically, however, they are more vulnerable than Millennials were: Rates of teen depression and suicide have skyrocketed since 2011. It’s not an exaggeration to describe iGen as being on the brink of the worst mental-health crisis in decades. Much of this deterioration can be traced to their phones.
Even when a seismic event—a war, a technological leap, a free concert in the mud—plays an outsize role in shaping a group of young people, no single factor ever defines a generation. Parenting styles continue to change, as do school curricula and culture, and these things matter. But the twin rise of the smartphone and social media has caused an earthquake of a magnitude we’ve not seen in a very long time, if ever. There is compelling evidence that the devices we’ve placed in young people’s hands are having profound effects on their lives—and making them seriously unhappy.
In the early 1970s, the photographer Bill Yates shot a series of portraits at the Sweetheart Roller Skating Rink in Tampa, Florida. In one, a shirtless teen stands with a large bottle of peppermint schnapps stuck in the waistband of his jeans. In another, a boy who looks no older than 12 poses with a cigarette in his mouth. The rink was a place where kids could get away from their parents and inhabit a world of their own, a world where they could drink, smoke, and make out in the backs of their cars. In stark black-and-white, the adolescent Boomers gaze at Yates’s camera with the self-confidence born of making your own choices—even if, perhaps especially if, your parents wouldn’t think they were the right ones.
Fifteen years later, during my own teenage years as a member of Generation X, smoking had lost some of its romance, but independence was definitely still in. My friends and I plotted to get our driver’s license as soon as we could, making DMV appointments for the day we turned 16 and using our newfound freedom to escape the confines of our suburban neighborhood. Asked by our parents, “When will you be home?,” we replied, “When do I have to be?”
But the allure of independence, so powerful to previous generations, holds less sway over today’s teens, who are less likely to leave the house without their parents. The shift is stunning: 12th-graders in 2015 were going out less often than eighth-graders did as recently as 2009.
Today’s teens are also less likely to date. The initial stage of courtship, which Gen Xers called “liking” (as in “Ooh, he likes you!”), kids now call “talking”—an ironic choice for a generation that prefers texting to actual conversation. After two teens have “talked” for a while, they might start dating. But only about 56 percent of high-school seniors in 2015 went out on dates; for Boomers and Gen Xers, the number was about 85 percent.
The decline in dating tracks with a decline in sexual activity. The drop is the sharpest for ninth-graders, among whom the number of sexually active teens has been cut by almost 40 percent since 1991. The average teen now has had sex for the first time by the spring of 11th grade, a full year later than the average Gen Xer. Fewer teens having sex has contributed to what many see as one of the most positive youth trends in recent years: The teen birth rate hit an all-time low in 2016, down 67 percent since its modern peak, in 1991.
Even driving, a symbol of adolescent freedom inscribed in American popular culture, from Rebel Without a Cause to Ferris Bueller’s Day Off, has lost its appeal for today’s teens. Nearly all Boomer high-school students had their driver’s license by the spring of their senior year; more than one in four teens today still lack one at the end of high school. For some, Mom and Dad are such good chauffeurs that there’s no urgent need to drive. “My parents drove me everywhere and never complained, so I always had rides,” a 21-year-old student in San Diego told me. “I didn’t get my license until my mom told me I had to because she could not keep driving me to school.” She finally got her license six months after her 18th birthday. In conversation after conversation, teens described getting their license as something to be nagged into by their parents—a notion that would have been unthinkable to previous generations.
Independence isn’t free—you need some money in your pocket to pay for gas, or for that bottle of schnapps. In earlier eras, kids worked in great numbers, eager to finance their freedom or prodded by their parents to learn the value of a dollar. But iGen teens aren’t working (or managing their own money) as much. In the late 1970s, 77 percent of high-school seniors worked for pay during the school year; by the mid-2010s, only 55 percent did. The number of eighth-graders who work for pay has been cut in half. These declines accelerated during the Great Recession, but teen employment has not bounced back, even though job availability has.
Of course, putting off the responsibilities of adulthood is not an iGen innovation. Gen Xers, in the 1990s, were the first to postpone the traditional markers of adulthood. Young Gen Xers were just about as likely to drive, drink alcohol, and date as young Boomers had been, and more likely to have sex and get pregnant as teens. But as they left their teenage years behind, Gen Xers married and started careers later than their Boomer predecessors had.
Gen X managed to stretch adolescence beyond all previous limits: Its members started becoming adults earlier and finished becoming adults later. Beginning with Millennials and continuing with iGen, adolescence is contracting again—but only because its onset is being delayed. Across a range of behaviors—drinking, dating, spending time unsupervised— 18-year-olds now act more like 15-year-olds used to, and 15-year-olds more like 13-year-olds. Childhood now stretches well into high school.
Why are today’s teens waiting longer to take on both the responsibilities and the pleasures of adulthood? Shifts in the economy, and parenting, certainly play a role. In an information economy that rewards higher education more than early work history, parents may be inclined to encourage their kids to stay home and study rather than to get a part-time job. Teens, in turn, seem to be content with this homebody arrangement—not because they’re so studious, but because their social life is lived on their phone. They don’t need to leave home to spend time with their friends.
If today’s teens were a generation of grinds, we’d see that in the data. But eighth-, 10th-, and 12th-graders in the 2010s actually spend less time on homework than Gen X teens did in the early 1990s. (High-school seniors headed for four-year colleges spend about the same amount of time on homework as their predecessors did.) The time that seniors spend on activities such as student clubs and sports and exercise has changed little in recent years. Combined with the decline in working for pay, this means iGen teens have more leisure time than Gen X teens did, not less.
So what are they doing with all that time? They are on their phone, in their room, alone and often distressed.
Jasu Hu
One of the ironies of iGen life is that despite spending far more time under the same roof as their parents, today’s teens can hardly be said to be closer to their mothers and fathers than their predecessors were. “I’ve seen my friends with their families—they don’t talk to them,” Athena told me. “They just say ‘Okay, okay, whatever’ while they’re on their phones. They don’t pay attention to their family.” Like her peers, Athena is an expert at tuning out her parents so she can focus on her phone. She spent much of her summer keeping up with friends, but nearly all of it was over text or Snapchat. “I’ve been on my phone more than I’ve been with actual people,” she said. “My bed has, like, an imprint of my body.”
In this, too, she is typical. The number of teens who get together with their friends nearly every day dropped by more than 40 percent from 2000 to 2015; the decline has been especially steep recently. It’s not only a matter of fewer kids partying; fewer kids are spending time simply hanging out. That’s something most teens used to do: nerds and jocks, poor kids and rich kids, C students and A students. The roller rink, the basketball court, the town pool, the local necking spot—they’ve all been replaced by virtual spaces accessed through apps and the web.
You might expect that teens spend so much time in these new spaces because it makes them happy, but most data suggest that it does not. The Monitoring the Future survey, funded by the National Institute on Drug Abuse and designed to be nationally representative, has asked 12th-graders more than 1,000 questions every year since 1975 and queried eighth- and 10th-graders since 1991. The survey asks teens how happy they are and also how much of their leisure time they spend on various activities, including nonscreen activities such as in-person social interaction and exercise, and, in recent years, screen activities such as using social media, texting, and browsing the web. The results could not be clearer: Teens who spend more time than average on screen activities are more likely to be unhappy, and those who spend more time than average on nonscreen activities are more likely to be happy.
There’s not a single exception. All screen activities are linked to less happiness, and all nonscreen activities are linked to more happiness. Eighth-graders who spend 10 or more hours a week on social media are 56 percent more likely to say they’re unhappy than those who devote less time to social media. Admittedly, 10 hours a week is a lot. But those who spend six to nine hours a week on social media are still 47 percent more likely to say they are unhappy than those who use social media even less. The opposite is true of in-person interactions. Those who spend an above-average amount of time with their friends in person are 20 percent less likely to say they’re unhappy than those who hang out for a below-average amount of time.
If you were going to give advice for a happy adolescence based on this survey, it would be straightforward: Put down the phone, turn off the laptop, and do something—anything—that does not involve a screen. Of course, these analyses don’t unequivocally prove that screen time causes unhappiness; it’s possible that unhappy teens spend more time online. But recent research suggests that screen time, in particular social-media use, does indeed cause unhappiness. One study asked college students with a Facebook page to complete short surveys on their phone over the course of two weeks. They’d get a text message with a link five times a day, and report on their mood and how much they’d used Facebook. The more they’d used Facebook, the unhappier they felt, but feeling unhappy did not subsequently lead to more Facebook use.
Social-networking sites like Facebook promise to connect us to friends. But the portrait of iGen teens emerging from the data is one of a lonely, dislocated generation. Teens who visit social-networking sites every day but see their friends in person less frequently are the most likely to agree with the statements “A lot of times I feel lonely,” “I often feel left out of things,” and “I often wish I had more good friends.” Teens’ feelings of loneliness spiked in 2013 and have remained high since.
This doesn’t always mean that, on an individual level, kids who spend more time online are lonelier than kids who spend less time online. Teens who spend more time on social media also spend more time with their friends in person, on average—highly social teens are more social in both venues, and less social teens are less so. But at the generational level, when teens spend more time on smartphones and less time on in-person social interactions, loneliness is more common.
So is depression. Once again, the effect of screen activities is unmistakable: The more time teens spend looking at screens, the more likely they are to report symptoms of depression. Eighth-graders who are heavy users of social media increase their risk of depression by 27 percent, while those who play sports, go to religious services, or even do homework more than the average teen cut their risk significantly.
Teens who spend three hours a day or more on electronic devices are 35 percent more likely to have a risk factor for suicide, such as making a suicide plan. (That’s much more than the risk related to, say, watching TV.) One piece of data that indirectly but stunningly captures kids’ growing isolation, for good and for bad: Since 2007, the homicide rate among teens has declined, but the suicide rate has increased. As teens have started spending less time together, they have become less likely to kill one another, and more likely to kill themselves. In 2011, for the first time in 24 years, the teen suicide rate was higher than the teen homicide rate.
Depression and suicide have many causes; too much technology is clearly not the only one. And the teen suicide rate was even higher in the 1990s, long before smartphones existed. Then again, about four times as many Americans now take antidepressants, which are often effective in treating severe depression, the type most strongly linked to suicide.
What’s the connection between smartphones and the apparent psychological distress this generation is experiencing? For all their power to link kids day and night, social media also exacerbate the age-old teen concern about being left out. Today’s teens may go to fewer parties and spend less time together in person, but when they do congregate, they document their hangouts relentlessly—on Snapchat, Instagram, Facebook. Those not invited to come along are keenly aware of it. Accordingly, the number of teens who feel left out has reached all-time highs across age groups. Like the increase in loneliness, the upswing in feeling left out has been swift and significant.
This trend has been especially steep among girls. Forty-eight percent more girls said they often felt left out in 2015 than in 2010, compared with 27 percent more boys. Girls use social media more often, giving them additional opportunities to feel excluded and lonely when they see their friends or classmates getting together without them. Social media levy a psychic tax on the teen doing the posting as well, as she anxiously awaits the affirmation of comments and likes. When Athena posts pictures to Instagram, she told me, “I’m nervous about what people think and are going to say. It sometimes bugs me when I don’t get a certain amount of likes on a picture.”
Girls have also borne the brunt of the rise in depressive symptoms among today’s teens. Boys’ depressive symptoms increased by 21 percent from 2012 to 2015, while girls’ increased by 50 percent—more than twice as much. The rise in suicide, too, is more pronounced among girls. Although the rate increased for both sexes, three times as many 12-to-14-year-old girls killed themselves in 2015 as in 2007, compared with twice as many boys. The suicide rate is still higher for boys, in part because they use more-lethal methods, but girls are beginning to close the gap.
These more dire consequences for teenage girls could also be rooted in the fact that they’re more likely to experience cyberbullying. Boys tend to bully one another physically, while girls are more likely to do so by undermining a victim’s social status or relationships. Social media give middle- and high-school girls a platform on which to carry out the style of aggression they favor, ostracizing and excluding other girls around the clock.
Social-media companies are of course aware of these problems, and to one degree or another have endeavored to prevent cyberbullying. But their various motivations are, to say the least, complex. A recently leaked Facebook document indicated that the company had been touting to advertisers its ability to determine teens’ emotional state based on their on-site behavior, and even to pinpoint “moments when young people need a confidence boost.” Facebook acknowledged that the document was real, but denied that it offers “tools to target people based on their emotional state.”
In July 2014, a 13-year-old girl in North Texas woke to the smell of something burning. Her phone had overheated and melted into the sheets. National news outlets picked up the story, stoking readers’ fears that their cellphone might spontaneously combust. To me, however, the flaming cellphone wasn’t the only surprising aspect of the story. Why, I wondered, would anyone sleep with her phone beside her in bed? It’s not as though you can surf the web while you’re sleeping. And who could slumber deeply inches from a buzzing phone?
Curious, I asked my undergraduate students at San Diego State University what they do with their phone while they sleep. Their answers were a profile in obsession. Nearly all slept with their phone, putting it under their pillow, on the mattress, or at the very least within arm’s reach of the bed. They checked social media right before they went to sleep, and reached for their phone as soon as they woke up in the morning (they had to—all of them used it as their alarm clock). Their phone was the last thing they saw before they went to sleep and the first thing they saw when they woke up. If they woke in the middle of the night, they often ended up looking at their phone. Some used the language of addiction. “I know I shouldn’t, but I just can’t help it,” one said about looking at her phone while in bed. Others saw their phone as an extension of their body—or even like a lover: “Having my phone closer to me while I’m sleeping is a comfort.”
It may be a comfort, but the smartphone is cutting into teens’ sleep: Many now sleep less than seven hours most nights. Sleep experts say that teens should get about nine hours of sleep a night; a teen who is getting less than seven hours a night is significantly sleep deprived. Fifty-seven percent more teens were sleep deprived in 2015 than in 1991. In just the four years from 2012 to 2015, 22 percent more teens failed to get seven hours of sleep.
The increase is suspiciously timed, once again starting around when most teens got a smartphone. Two national surveys show that teens who spend three or more hours a day on electronic devices are 28 percent more likely to get less than seven hours of sleep than those who spend fewer than three hours, and teens who visit social-media sites every day are 19 percent more likely to be sleep deprived. A meta-analysis of studies on electronic-device use among children found similar results: Children who use a media device right before bed are more likely to sleep less than they should, more likely to sleep poorly, and more than twice as likely to be sleepy during the day.
Electronic devices and social media seem to have an especially strong ability to disrupt sleep. Teens who read books and magazines more often than the average are actually slightly less likely to be sleep deprived—either reading lulls them to sleep, or they can put the book down at bedtime. Watching TV for several hours a day is only weakly linked to sleeping less. But the allure of the smartphone is often too much to resist.
Sleep deprivation is linked to myriad issues, including compromised thinking and reasoning, susceptibility to illness, weight gain, and high blood pressure. It also affects mood: People who don’t sleep enough are prone to depression and anxiety. Again, it’s difficult to trace the precise paths of causation. Smartphones could be causing lack of sleep, which leads to depression, or the phones could be causing depression, which leads to lack of sleep. Or some other factor could be causing both depression and sleep deprivation to rise. But the smartphone, its blue light glowing in the dark, is likely playing a nefarious role.
The correlations between depression and smartphone use are strong enough to suggest that more parents should be telling their kids to put down their phone. As the technology writer Nick Bilton has reported, it’s a policy some Silicon Valley executives follow. Even Steve Jobs limited his kids’ use of the devices he brought into the world.
What’s at stake isn’t just how kids experience adolescence. The constant presence of smartphones is likely to affect them well into adulthood. Among people who suffer an episode of depression, at least half become depressed again later in life. Adolescence is a key time for developing social skills; as teens spend less time with their friends face-to-face, they have fewer opportunities to practice them. In the next decade, we may see more adults who know just the right emoji for a situation, but not the right facial expression.
I realize that restricting technology might be an unrealistic demand to impose on a generation of kids so accustomed to being wired at all times. My three daughters were born in 2006, 2009, and 2012. They’re not yet old enough to display the traits of iGen teens, but I have already witnessed firsthand just how ingrained new media are in their young lives. I’ve observed my toddler, barely old enough to walk, confidently swiping her way through an iPad. I’ve experienced my 6-year-old asking for her own cellphone. I’ve overheard my 9-year-old discussing the latest app to sweep the fourth grade. Prying the phone out of our kids’ hands will be difficult, even more so than the quixotic efforts of my parents’ generation to get their kids to turn off MTV and get some fresh air. But more seems to be at stake in urging teens to use their phone responsibly, and there are benefits to be gained even if all we instill in our children is the importance of moderation. Significant effects on both mental health and sleep time appear after two or more hours a day on electronic devices. The average teen spends about two and a half hours a day on electronic devices. Some mild boundary-setting could keep kids from falling into harmful habits.
In my conversations with teens, I saw hopeful signs that kids themselves are beginning to link some of their troubles to their ever-present phone. Athena told me that when she does spend time with her friends in person, they are often looking at their device instead of at her. “I’m trying to talk to them about something, and they don’t actually look at my face,” she said. “They’re looking at their phone, or they’re looking at their Apple Watch.” “What does that feel like, when you’re trying to talk to somebody face-to-face and they’re not looking at you?,” I asked. “It kind of hurts,” she said. “It hurts. I know my parents’ generation didn’t do that. I could be talking about something super important to me, and they wouldn’t even be listening.”
Once, she told me, she was hanging out with a friend who was texting her boyfriend. “I was trying to talk to her about my family, and what was going on, and she was like, ‘Uh-huh, yeah, whatever.’ So I took her phone out of her hands and I threw it at my wall.”
I couldn’t help laughing. “You play volleyball,” I said. “Do you have a pretty good arm?” “Yep,” she replied.
What I Needed From the Church During My Depression
3 ways our communities can support mental health.
Alicia Cohn | posted August 3, 2016
Image: Milos Kreckovic / iStock
Speaking at the Democratic National Convention last week, the singer Demi Lovato took advantage of the powerful platform to advocate for mental health care in America. “Like millions of Americans, I am living with mental illness,” she said. "Too many Americans from all walks of life don't get help, either because they fear the stigma or they cannot afford treatment."
“Mental illness” is a scary-sounding category that encompasses a broad array of invisible struggles. Look around you on Sunday. Most likely, there are Christians next to you suffering silently from anxiety or panic disorder, bipolar disorder (from which Lovato suffers), dysthymia or major depressive disorder (from which I have suffered). Whether through personal experience or through someone we know, those of us whose lives have been touched by mental health struggles know that getting help can be the hardest part.
Women are twice as likely to experience mental health struggles as men, thanks to major hormonal challenges such as pregnancy and menstruation. According to the Centers for Disease Control and Prevention (CDC), 30 percent of women between 18 and 44 years of age are affected by depression, and many of them don’t get the help they need. (My own disorder went undiagnosed for almost six months before I got help from doctors and therapy, and even then, the recovery process has been hindered by bad advice, mistreatment, and poor choices about whom I can rely on.)
Unfortunately, many of us who have spoken up in church communities have been told to “pray harder” or “have more faith.” These suggestions might be well intentioned, but they often discourage and isolate those of us in desperate need of support. “It’s a knee-jerk reaction to judge people when they’re vulnerable,” wrote actress Kristen Bell of her own story. “But there’s nothing weak about struggling with mental illness. You’re just having a harder time living in your brain than other people.”
She’s right: Struggling with an illness of any kind makes a person vulnerable, and a sick brain puts a person in a particularly vulnerable state because it’s often impossible to discern the problem from the inside. The sick brain can’t see the sick brain. More often than not, someone in the midst of a depressive episode or panic attack can barely put forth a cry for help.
As people living in Christian community, we should be ready to offer practical knowledge and gracious support to people experiencing mental health crises. With that in mind, here are three ways I believe every church is best positioned to help:
Faith in something better.
“Have faith that on the other side of your pain is something good,” Dwayne “The Rock” Johnson told the Oprah Presents Master Class. He wished someone had relayed this idea to him during a low point in his life when he was “crying constantly.” His message mirrors the “It gets better” campaign, but many people suffering from depression or other mental health issues know that sometimes it gets worse. Everyone needs a reason to keep trying. I’ve been in enough therapy groups and doctors’ offices to know that the only reason people keep looking for answers in the face of crippling despair is because they believe something will help: drugs, doctors, relationships, therapy, or sometimes the sheer freedom of living at rock bottom. Nonetheless, I've seen the best results when I (and others) put faith not exclusively in doctors or drugs or therapies, which have their limits, but also in God. He is the reason I still believe in “something good” on the other side of my pain.
If you know someone in your church like me who is suffering, come alongside her. Pray for her. Avoid cheap platitudes like “have faith” and instead offer practical support by checking in on a regular basis to let her know she’s not alone, or by asking about her treatment, which is a way of acknowledging that the illness is real.
Resilience.
Millennials are on more antidepressants than any other generation. According to the CDC, more than 6 percent of 18-to 39-year-olds have been prescribed antidepressants. My generation might as well define ourselves as “behind” in our careers (40 percent of unemployed people are milennials), salaries, and personal lives (marrying late and moving back in with our parents). No wonder we’re depressed. On top of that, the hours we spend in psychiatrists’ or counselors’ offices dealing with symptoms of a disorder (or the side effects of medication) often feel like “lost” time. While dealing with my mental health problems, I have burned through a lot of time and money as well as emotional and relationship capital—all resources that I feel could have been spent better elsewhere. I find it reassuring to know that Christianity offers a promise of restoration greater than anything lost (Joel 2:25; Job 42:10–17). In the Bible, people often fall down, their lives fall apart, and yet God raises them up again.
With that in mind, if you encounter someone in your church who is struggling with suicidal ideation or any form of hopelessness, first affirm their pain, then offer them the grace of optimism.
The "seasonal" perspective.
“For now” is the mantra my therapist gave me to get through depressive episodes and hard days. Ecclesiastes 3 provides a similar mantra: “To everything there is a season.” Mental health, too, is composed of seasons. I am currently in a season for antidepressants, and although it may be cyclical, I hope it will eventually end. For most people, circumstances change, the brain’s reactions change accordingly, and the appropriate therapy also changes in sync with the situation. With mental health challenges, maintaining a long-range perspective is key to survival. The hardest, most important thing to do is simply to persevere.
If someone near you is facing a discrete mental health episode or a lifelong challenge, encourage her to name the season she’s in, remind her that seasons often change, and journey with her as she takes it one day at a time.
“I don't think I'm fixed,” Lovato shared in the MTV documentary about her “recovery” in a residential treatment facility. “People think that you're like a car in a body shop. You go in, they fix you, and you're out. It takes constant fixing."
Much like spiritual health, mental health is an ongoing need for every human being. Although those of us who struggle are each responsible for ourselves, we also rely on the powerful support of our community to ensure that we get the care we need. It starts with awareness within each local church. Just as an increasing number of secular figures have spoken up publicly, Christians should step forward to be, as Lovato put it, “proof that you can live a normal and empowered life with mental illness.”
The Bible is filled with exhortations to care for the most vulnerable among us—those who cry out for mercy and feel they have nowhere to turn. Those of us who face mental health crises are among the most vulnerable. We need your recognition. We need your prayers. We need your presence. And we need to be part of the church community, especially as we struggle to find extra grace.
The idea that one’s sex is a feeling, not a fact, has permeated our culture and is leaving casualties in its wake. Gender dysphoria should be treated with psychotherapy, not surgery.
For forty years as the University Distinguished Service Professor of Psychiatry at Johns Hopkins Medical School—twenty-six of which were also spent as Psychiatrist in Chief of Johns Hopkins Hospital—I’ve been studying people who claim to be transgender. Over that time, I’ve watched the phenomenon change and expand in remarkable ways.
A rare issue of a few men—both homosexual and heterosexual men, including some who sought sex-change surgery because they were erotically aroused by the thought or image of themselves as women—has spread to include women as well as men. Even young boys and girls have begun to present themselves as of the opposite sex. Over the last ten or fifteen years, this phenomenon has increased in prevalence, seemingly exponentially. Now, almost everyone has heard of or met such a person.
Publicity, especially from early examples such as “Christine” Jorgenson, “Jan” Morris, and “Renee” Richards, has promoted the idea that one’s biological sex is a choice, leading to widespread cultural acceptance of the concept. And, that idea, quickly accepted in the 1980s, has since run through the American public like a revelation or “meme” affecting much of our thought about sex.
The champions of this meme, encouraged by their alliance with the broader LGBT movement, claim that whether you are a man or a woman, a boy or a girl, is more of a disposition or feeling about yourself than a fact of nature. And, much like any other feeling, it can change at any time, and for all sorts of reasons. Therefore, no one could predict who would swap this fact of their makeup, nor could one justifiably criticize such a decision.
At Johns Hopkins, after pioneering sex-change surgery, we demonstrated that the practice brought no important benefits. As a result, we stopped offering that form of treatment in the 1970s. Our efforts, though, had little influence on the emergence of this new idea about sex, or upon the expansion of the number of “transgendered” among young and old.
Olympic Athlete Turned "Pin-Up" Girl
This history may clarify some aspects of the latest high-profile transgender claimant. Bruce Jenner, the 1976 Olympic decathlon champion, is turning away from his titular identity as one of the “world’s greatest male athletes.” Jenner announced recently that he “identifies as a woman” and, with medical and surgical help, is busy reconstructing his physique.
I have not met or examined Jenner, but his behavior resembles that of some of the transgender males we have studied over the years. These men wanted to display themselves in sexy ways, wearing provocative female garb. More often than not, while claiming to be a woman in a man’s body, they declared themselves to be “lesbians” (attracted to other women). The photograph of the posed, corseted, breast-boosted Bruce Jenner (a man in his mid-sixties, but flaunting himself as if a “pin-up” girl in her twenties or thirties) on the cover of Vanity Fair suggests that he may fit the behavioral mold that Ray Blanchard has dubbed an expression of “autogynephilia”—from gynephilia (attracted to women) and auto (in the form of oneself).
The Emperor’s New Clothes
But the meme—that your sex is a feeling, not a biological fact, and can change at any time—marches on through our society. In a way, it’s reminiscent of the Hans Christian Andersen tale, The Emperor’s New Clothes. In that tale, the Emperor, believing that he wore an outfit of special beauty imperceptible to the rude or uncultured, paraded naked through his town to the huzzahs of courtiers and citizens anxious about their reputations. Many onlookers to the contemporary transgender parade, knowing that a disfavored opinion is worse than bad taste today, similarly fear to identify it as a misapprehension.
I am ever trying to be the boy among the bystanders who points to what’s real. I do so not only because truth matters, but also because overlooked amid the hoopla—enhanced now by Bruce Jenner’s celebrity and Annie Leibovitz’s photography—stand many victims. Think, for example, of the parents whom no one—not doctors, schools, nor even churches—will help to rescue their children from these strange notions of being transgendered and the problematic lives these notions herald. These youngsters now far outnumber the Bruce Jenner type of transgender. Although they may be encouraged by his public reception, these children generally come to their ideas about their sex not through erotic interests but through a variety of youthful psychosocial conflicts and concerns.
First, though, let us address the basic assumption of the contemporary parade: the idea that exchange of one’s sex is possible. It, like the storied Emperor, is starkly, nakedly false. Transgendered men do not become women, nor do transgendered women become men. All (including Bruce Jenner) become feminized men or masculinized women, counterfeits or impersonators of the sex with which they “identify.” In that lies their problematic future.
When “the tumult and shouting dies,” it proves not easy nor wise to live in a counterfeit sexual garb. The most thorough follow-up of sex-reassigned people—extending over thirty years and conducted in Sweden, where the culture is strongly supportive of the transgendered—documents their lifelong mental unrest. Ten to fifteen years after surgical reassignment, the suicide rate of those who had undergone sex-reassignment surgery rose to twenty times that of comparable peers.
How to Treat Gender Dysphoria
So how should we make sense of this matter today? As with any mental phenomenon, what’s crucial is noting its fundamental characteristic and then identifying the many ways in which that characteristic can manifest itself.
The central issue with all transgender subjects is one of assumption—the assumption that one’s sexual nature is misaligned with one’s biological sex. This problematic assumption comes about in several different ways, and these distinctions in its generation determine how to manage and treat it.
Based on the photographic evidence one might guess Bruce Jenner falls into the group of men who come to their disordered assumption through being sexually aroused by the image of themselves as women. He could have been treated for this misaligned arousal with psychotherapy and medication. Instead, he found his way to surgeons who worked him over as he wished. Others have already commented on his stereotypic caricature of women as decorative “babes” (“I look forward to wearing nail polish until it chips off,” he said to Diane Sawyer)—a view that understandably infuriates feminists—and his odd sense that only feelings, not facts, matter here.
For his sake, however, I do hope that he receives regular, attentive follow-up care, as his psychological serenity in the future is doubtful. Future men with similar feelings and intentions should be treated for those feelings rather than being encouraged to undergo bodily changes. Group therapies are now available for them.
Most young boys and girls who come seeking sex-reassignment are utterly different from Jenner. They have no erotic interest driving their quest. Rather, they come with psychosocial issues—conflicts over the prospects, expectations, and roles that they sense are attached to their given sex—and presume that sex-reassignment will ease or resolve them.
The grim fact is that most of these youngsters do not find therapists willing to assess and guide them in ways that permit them to work out their conflicts and correct their assumptions. Rather, they and their families find only “gender counselors” who encourage them in their sexual misassumptions.
Those with Gender Dysphoria Need Evidence-Based Care
There are several reasons for this absence of coherence in our mental health system. Important among them is the fact that both the state and federal governments are actively seeking to block any treatments that can be construed as challenging the assumptions and choices of transgendered youngsters. “As part of our dedication to protecting America’s youth, this administration supports efforts to ban the use of conversion therapy for minors,” said Valerie Jarrett, a senior advisor to President Obama.
In two states, a doctor who would look into the psychological history of a transgendered boy or girl in search of a resolvable conflict could lose his or her license to practice medicine. By contrast, such a physician would not be penalized if he or she started such a patient on hormones that would block puberty and might stunt growth.
What is needed now is public clamor for coherent science—biological and therapeutic science—examining the real effects of these efforts to “support” transgendering. Although much is made of a rare “intersex” individual, no evidence supports the claim that people such as Bruce Jenner have a biological source for their transgender assumptions. Plenty of evidence demonstrates that with him and most others, transgendering is a psychological rather than a biological matter.
In fact, gender dysphoria—the official psychiatric term for feeling oneself to be of the opposite sex—belongs in the family of similarly disordered assumptions about the body, such as anorexia nervosa and body dysmorphic disorder. Its treatment should not be directed at the body as with surgery and hormones any more than one treats obesity-fearing anorexic patients with liposuction. The treatment should strive to correct the false, problematic nature of the assumption and to resolve the psychosocial conflicts provoking it. With youngsters, this is best done in family therapy.
The larger issue is the meme itself. The idea that one’s sex is fluid and a matter open to choice runs unquestioned through our culture and is reflected everywhere in the media, the theater, the classroom, and in many medical clinics. It has taken on cult-like features: its own special lingo, internet chat rooms providing slick answers to new recruits, and clubs for easy access to dresses and styles supporting the sex change. It is doing much damage to families, adolescents, and children and should be confronted as an opinion without biological foundation wherever it emerges.
But gird your loins if you would confront this matter. Hell hath no fury like a vested interest masquerading as a moral principle.
Paul McHugh, MD, is University Distinguished Service Professor of Psychiatry at Johns Hopkins Medical School and the former psychiatrist in chief at Johns Hopkins Hospital. He is the author of The Mind Has Mountains: Reflections on Society and Psychiatry.
When I was 15 years old, my mother picked me up at school to take me to a dental appointment. In the car, I could tell immediately that she wasn't functioning normally—she was headed for another "episode." She drove nervously, struggling to recognize her surroundings. She was silent except when I forced conversation, and when she did speak, her speech was slow and seemed to require deliberation.
It was as if half of her had already shrunk into some unknown place, and the other half was not sure whether to follow or to maintain her grip on the reality of her daughter and a trip to the dentist.
I asked Mom if she had taken her medication that day. Her answer was not straightforward, but it was clear that she was not fully medicated and stable. So with one part of my brain, I prayed for a safe trip to the dentist. With another part, I employed a technique used by many people who feel powerless in the face of an unnamed enemy: I acted as if nothing was wrong.
At the dentist's office, when my name was called, I left my mother in the waiting room and went back for my appointment. After half an hour or so with the dentist, I returned to my mom, who didn't look at me.
"Mom, it's time to go," I said. "I'm finished." I received no response of any kind. Suddenly I realized my instincts had been right: something indeed was wrong with Mom … again. And it was up to me to help her.
I touched her arm and gently tried to shake her back to awareness, with no results. She was rigidly catatonic, immovable, staring into space and clutching her purse in her lap with clenched hands—in a waiting room full of strangers.
After a couple of quiet attempts to rouse her, I began to attract attention. People stared at me as I tried to get her to respond. When she wouldn't move, I realized I needed to call my dad at work for help.
As everyone in the room continued to stare, I walked to the reception desk and asked the woman behind the counter—who was also staring—if I could use the phone.
"No, there's a pay phone around the corner," she said. When I explained that I needed to call my dad for help, I didn't have change for the phone, and it would be a local call, she still refused. So I went back to my mom and wrestled with her rigid arms, pulling them aside enough to get into her purse to find a quarter for the phone. I went back to the receptionist to ask if she could keep an eye on my mom while I went to use the pay phone. She shrunk back in horror: "Is she dangerous?"
After assuring the receptionist that my motionless mother was not about to attack her, I called my dad and then returned to sit next to my mom till he got there. The receptionist and the people in the waiting room took turns staring at my mom, glancing at me, and studying the floor. No one asked if I needed help.
In the years since, that incident has become for me a symbol. The way people in that waiting room responded to my family's public crisis is the way I've seen people—including those in the church—respond to serious mental illness. They didn't know what to do for my mom or anyone associated with her. So they did nothing.
Though I didn't know it at the time, my mother has schizophrenia. As often happens with schizophrenics, she had not been faithfully taking her anti-psychotic drugs and had lost touch with reality. Dad and I took her to the hospital for another of her psychiatric stays and restabilization on medication.
I have been doing a lot of thinking about session length lately. Over the past several years I have followed the trend of decreasing my session length to 45 minutes. I remember when sessions were standardized at 50 minutes when I started practicing 36 years ago. The idea was to see people for 50 minutes then have a 10 minute break between sessions, which worked pretty well for most people. Intakes were a little difficult to fit in that time for most people and often needed a longer time period. The biggest challenge was couples. Trying to fit a session with a couple into 50 minutes was always difficult and fitting them into 45 minutes, which is now the standard time that third party reimbursers ususally pay for, is even harder.
So with that in mind I thought I would adjust session length to 75 minutes to 90 minutes. Seventy-five minutes seems to work much better with most of the people I would with including couples and individuals and we don't seem rushed. Then I have 15 minutes between sessions if needed. People seem to treat time differently. Previously most of my clients came for weekly sessions but now they tend to come biweekly or longer, which actually works better for most people and especially couples giving them time to work on issues between sessions.
From a financial perspective it is more economical for clients to come less frequently and be seen longer at each session since I charge the same for 75 minute to 90 minute sessions as I used to charge for 45 minute sessions. I suppose I could charge more but I would rather take my time with each couple or individual and pass the cost savings on to them. For them it is like they get two sessions for the price of one each time and I get the luxury of a longer amount of their time when I have them, which is especially helpful since it is often difficult for clients and espeically couples to find time to be a couple let alone come for counseling.
I have also noticed the relaxed pace helps both me and my clients relax as well. I am not as sensitive to watching the time and being careful not to cross into the next session. This makes sessions seem rushed and often results in items getting moved to the next session, which due to client's time constraints may not occur with the frequence it once did.
This process may not work for all counselors but I find it effective for me and the folks I work with.
The leading Christian scholar on gender dysphoria defines the terms—and gives the church a way forward.
Mark Yarhouse / posted June 8, 2015
Image: Tom Maday
I still recall one of my first meetings with Sara. Sara is a Christian who was born male and named Sawyer by her parents. As an adult, Sawyer transitioned to female.
Sara would say transitioning—adopting a cross-gender identity—took 25 years. It began with facing the conflict she experienced between her biology and anatomy as male, and her inward experience as female. While still Sawyer, she would grow her hair out, wear light makeup, and dress in feminine attire from time to time. She also met with what seemed like countless mental-health professionals as well as several pastors. For Sawyer, now Sara, transitioning eventually meant using hormones and undergoing sex reassignment surgery.
Sara would say she knew at a young age—around 5—that she was really a girl. Her parents didn’t know what to do. They hoped their son was just different from most other boys. Then they hoped it was a phase Sawyer would get through. Later, two pastors told them that their son’s gender identity conflicts were a sign of willful disobedience. They tried to discipline their son, to no avail.
Sara opened our first meeting by saying, “I may have sinned in the decisions I made; I’m not sure I did the right thing. At the time, I felt excruciating distress. I thought I would take my life. What would you have me do?” The exchange was disarming.
I have worked with people like Sara for more than 16 years. Although most of my published research and clinical practice is in the area of sexual identity, I regularly receive referrals to meet with people who experience conflicts like Sara’s. The research institute I direct, housed at Regent University in Virginia, published the first study of its kind on transgender Christians a few years ago. My experiences counseling children, adolescents, and adults have all compelled me to further study gender dysphoria.
From this research and counseling background, I hope to offer the Christian community a distinctly Christian response to gender dysphoria.
Defining the Terms
First, let’s define our terms. “Gender identity” is simply how people experience themselves as male or female, including how masculine or feminine they feel. “Gender dysphoria” refers to deep and abiding discomfort over the incongruence between one’s biological sex and one’s psychological and emotional experience of gender. Sara would say she lived much of her life as a woman trapped inside a man’s body. When a person reports gender identity concerns that cause significant distress, he or she may meet criteria for a gender dysphoria diagnosis.
The previous version of the American Psychiatric Association’s diagnostic manual included the diagnosis “gender identity disorder.” It highlighted cross-gender identity as the point of concern. The newest version refers instead to “gender dysphoria,” moving the discussion away from identity and toward the experience of distress. A lack of congruence between one’s biological sex and gender identity exists on a continuum, so when diagnosing gender dysphoria, mental-health professionals look at the amount of distress as well as the amount of impairment at work or in social settings.
Editor's Note: What's In a Pronoun
A brief word about the pronouns we use to identify the people in this article and "Loving My Sister-Brother."
As the experiences of transgender persons have come to light over the past several years, mainstream media have created guidelines for reporting on them. Following general journalistic practice, we at CT follow a simple rule: Use the pronoun that the person uses. For example, we refer to Sara—the person at the beginning of this essay—as a "she," because Sara identifies as one.
Yet for the first-person essay from Margaret Philbrick, we deliberated. Calling Philbrick's sibling a "he" risked insensitivity. Yet using "she" didn't accurately convey Philbrick's own conflicted experience. In the end, we kept the male pronoun, to underscore the tension the family faces in navigating this life change. Carly Lehwald, Philbrick's sibling, has given us permission to use the male pronoun for this particular story.
-The Editors
It is hard to know exactly how many people experience gender dysphoria. Most of the research has been on “transsexuality.” The term refers to a person like Sara who wishes to or has identified with the opposite sex, often through hormonal treatment or surgery. The American Psychiatric Association estimates the number of transsexual adults as low as 0.005 to 0.014 percent of men and 0.002 to 0.003 percent of women. But these are likely underestimates, as they are based on the number of people who visit specialty clinics.
The highest prevalence estimates come from more recent surveys that include “transgender” as an option. “Transgender” is an umbrella term for the many ways people experience a mismatch between their gender identity and their biological sex. So not everyone who is transgender experiences significant gender dysphoria. Some people say their gender resides along a continuum in between male and female or is fluid. They do not tend to report as much distress. Prevalence here has ranged from 1 in 215 to 1 in 300.
This means that transgender people are much more common than those formally diagnosed with gender dysphoria, but not nearly as common as those who identity as gay or lesbian, which is 2 to 4 percent of the US population.
While on the topic of homosexuality, let me clarify that gender dysphoria and transgender issues are not about having sex or attraction to the same sex; they are about an experiential mismatch between one’s psychology and one’s biology. People often confuse the two, likely due to transgender being a part of the larger lesbian, gay, bisexual, and transgender (LGBT) discussion.
Psychologists and researchers don’t know what causes gender dysphoria. The most popular theory among those who publish on this topic is the brain-sex theory. It proposes that the brain maps toward male or female, which in nearly all cases corresponds with various biological indicators of sex: chromosomes, gonads, and sex hormones. In rare instances, the normal sex differentiation that occurs in utero occurs in one direction (differentiating toward male, for example), while the brain maps in the other direction (toward female). Several gaps remain in the research behind this theory, but it nonetheless compels many professionals.
Recently a mother came to me, worried about her 7-year-old son. “What can we do?” she asked. “Just last week a woman at the park said something. I couldn’t believe she had the nerve. I’m afraid the kids at school might do worse.”
The mother noted that her son’s voice inflection seemed more like a girl’s and that he pretended he had long hair. Over the past weekend, he had grabbed a towel and put it around his waist and said, “Look, Mom, I’m wearing a dress just like you!”
Gender dysphoria and transgender issues are not about having sex or attraction to the same sex; they are about an experiential mismatch between one’s psychology and one’s biology.
Whether and how to intervene when a child is acting in ways typical of the opposite sex is a controversial topic, to say the least. It’s important to remember that in about three of four of these cases, the gender identity conflict resolves on its own, lessening or ceasing entirely. However, about three-fourths of children who experience a lessening or resolution go on as adults to identify as gay, lesbian, or bisexual—a fact that psychologists don’t fully understand at this time.
What happens to children when their gender identity conflict continues into adulthood? Psychiatrist Richard Carroll proposes that they face four outcomes: (1) live in accordance with one’s biological sex and gender role; (2) engage in cross-gender behavior intermittently; (3) adopt a cross-gender role through sex reassignment surgery; or (4) unresolved (the clinician has lost contact with the person and doesn’t know what happened).
Sara pursued the third outcome. Bert pursued the second. He’s a biological male who for years has engaged in cross-gender behavior from time to time to “manage” his gender dysphoria. He wears feminine undergarments that no one apart from his wife knows about. He has grown his hair out and may wear light makeup, and this has been enough to manage his dysphoria.
Crystal pursued the first option. She has experienced gender dysphoria since childhood. It has ebbed and flowed throughout her life, but she’s able to cope with it. She presents as a woman and has been married to a man for 12 years. He is aware of her dysphoria.
Few studies have shown that therapy successfully helps an adult with gender dysphoria resolve with their biological sex. This may be one reason professionals generally support some cross-gender identification in therapy.
As someone with gender dysphoria considers different ways to cope, what might the Christian community distinctly offer them?
Three Lenses
To answer this question, let me first describe three cultural lenses through which people tend to “see” gender dysphoria.
Lens #1: Integrity. The integrity lens views sex and gender and, therefore, gender identity in terms of what theologian Robert Gagnon refers to as “the sacred integrity of maleness or femaleness stamped on one’s body.” Cross-gender identification is a concern because it threatens to dishonor the creational order of male and female. Specific biblical passages, such as Deuteronomy 22:5 or 23:1, bolster this view. Even if we concede that some of the Old Testament prohibitions were related to avoiding pagan practices, nonetheless, from beginning to end, Scripture reflects the importance of male-female complementarity set forth in creation (Gen. 2:21–24).
The theological foundation of the integrity lens raises the same kind of concerns about cross-gender identification as it raises about homosexuality. Same-sex sexual behavior is sin in part because it doesn’t “merge or join two persons into an integrated sexual whole,” writes Gagnon. “Essential maleness” and “essential femaleness” are not brought together as intended from creation. When extended to transsexuality and cross-gender identification, the theological concerns rest in what Gagnon calls the “denial of the integrity of one’s own sex and an overt attempt at marring the sacred image of maleness or femaleness formed by God.”
The integrity lens most clearly reflects the biblical witness about sex and gender. While it may be challenging to identify a “line” in thought, behavior, and manner that reflects cross-gender identification, people who see through the integrity lens are concerned that cross-gender identification moves against the integrity of one’s biological sex—an essential aspect of personhood.
It should be noted that some Christians do not put gender dysphoria in the same category as homosexuality. They may have reservations about more invasive procedures; however, they do put gender dysphoria or trying to manage dysphoria in the same class of behaviors that Scripture deems immoral.
Lens #2: Disability. This lens views gender dysphoria as a result of living in a fallen world, but not a direct result of moral choice. Whether we accept brain-sex theory or another account of the origins of the phenomenon, if the various aspects of sex and gender are not aligning, then it’s one more human experience that is “not the way it’s supposed to be,” to borrow a phrase from theologian Cornelius Plantinga Jr.
When we care for someone suffering from depression or anxiety, we do not discuss their emotional state as a moral choice. Rather, the person simply contends with a condition that comes in light of the Fall. The person may have choices to make in response to the condition, and those choices have moral and ethical dimensions. But the person is not culpable for having the condition as such. Here, the parallel to people with gender dysphoria should be clear.
Those who use this lens seek to learn as much as they can from two key sources: special revelation (scriptural teachings on sex and gender) and general revelation (research on causes, prevention, and intervention, as well the lives of persons navigating gender dysphoria). This lens leads to the question: How should we respond to a condition with reference to the goodness of Creation, the reality of the Fall, and the hope of restoration?
Those drawn to the disability lens may value the sacredness of male and female differences; this is implied in calling gender dysphoria a disability. But the disability lens also makes room for supportive care and interventions that allow for cross-gender identification in a way the integrity lens does not.
Lens #3: Diversity. This lens sees the reality of transgender persons as something to be celebrated, honored, or revered. Our society is rapidly moving in this direction. Those drawn to this lens cite historical examples in which departures from a clear male-or-female presentation have been held in high esteem, such as the Fa’afafine of Samoan Polynesian culture.
Whereas the biological distinction between male and female is considered unchangeable, some wish to recast sex as just as socially constructed as gender. To evangelicals, those who want to deconstruct sex and gender norms represent a much more radical alternative to either the integrity or disability lens.
To be sure, not everyone drawn to the diversity lens wants to deconstruct sex and gender. What is perhaps most compelling about this lens is that it answers questions about identity—“Who am I?”—and community—“Of which community am I a part?” It answers the desire for persons with gender dysphoria to be accepted and to find purpose in their lives.
A Distinctly Christian Resource
I believe there are strengths in all three lenses. Because I am a psychologist who makes diagnoses and provides treatment to people experiencing gender dysphoria, I see value in a disability lens that sees gender dysphoria as a reflection of a fallen world in which the condition itself is not a moral choice. This helps me see the person facing gender identity confusion with empathy and compassion. I try to help the person manage his or her gender dysphoria.
When I consider how best to counsel my clients to manage their gender dysphoria, I add the caveat: in the least invasive way possible.
Even as Christians affirm the disability lens, we should also let the integrity lens inform our pastoral care. That lens represents a genuine concern for the integrity of sex and gender, and the ways in which maleness and femaleness help us understand the nature of the church and even the gospel.
Yet we should reject the teaching that gender identity conflicts are the result of willful disobedience or sinful choice. The church can be sensitive as questions arise about how best to manage gender dysphoria in light of the integrity lens. And we can recognize that we live in a specific cultural context, and that many gender roles vary from culture to culture. When I consider how best to counsel my clients to manage their gender dysphoria, however, I add the caveat: in the least invasive way possible.
Christians can also acknowledge how the diversity lens affirms the person by providing an identity not addressed by the other two lenses. The diversity lens emphasizes the importance of belonging. We must remember that the transgender and broader LGBT community are attractive because they answer the bedrock question, “Where do I belong?” Most churches want to be a community where people suffering from any “dysphoria” will feel they belong, for the church is, after all, a community of broken people saved by grace.
A few years ago, my research team at the Institute for the Study of Sexual Identity conducted the first study of its kind on transgender Christians. We collected information on 32 biological males who to varying degrees had transitioned to or presented as women. We asked many questions about issues they faced in their home, workplace, and church, such as, “What kind of support would you have liked from the church?” One person answered, “Someone to cry with me rather than just denounce me. Hey, it is scary to see God not rescue someone from cancer or schizophrenia or [gender dysphoria]...but learn to allow your compassion to overcome your fear and repulsion.”
When it comes to support, many evangelical communities may be tempted to respond to transgender persons by shouting “Integrity!” The integrity lens is important, but simply urging persons with gender dysphoria to act in accordance with their biological sex and ignore their extreme discomfort won’t constitute pastoral care or a meaningful cultural witness.
The disability lens may lead us to shout, “Compassion!” and the diversity lens may lead us to shout “Celebrate!” But both of these lenses suggest that the creational goodness of maleness and femaleness can be discarded—or that no meaning is to be found in the marks of our suffering.
Most centrally, the Christian community is a witness to the message of redemption. We are witnesses to redemption through Jesus’ presence in our lives. Redemption is not found by measuring how well a person’s gender identity aligns with their biological sex, but by drawing them to the person and work of Jesus Christ, and to the power of the Holy Spirit to transform us into his image.
Let’s say Sara walks into your church. She looks like a man dressed as a woman. One question she will be asking is, “Am I welcome here?”
As Christians speak to this redemption, we will be tempted to join in the culture wars about sex and gender that fall closely on the heels of the wars about sexual behavior and marriage. But in most cases, the church is called to rise above those wars and present a witness to redemption.
Let’s say Sara walks into your church. She looks like a man dressed as a woman. One question she will be asking is, “Am I welcome here?” In the spirit of a redemptive witness, I hope to communicate to her through my actions: “Yes, you are in the right place. We want you here.”
If I am drawn to a conversation or relationship with her, I hope to approach her not as a project, but as a person seeking real and sustained relationship, which is characterized by empathy as well as encouragement to walk faithfully with Christ. But I should not try to “fix” her, because unless I’m her professional therapist, I’m not privy to the best way to resolve her gender dysphoria. Rather, Christians are to foster the kinds of relationships that will help us know and love and obey Jesus better than we did yesterday. That is redemption.
If Sara shares her name with me, as a clinician and Christian, I use it. I do not use this moment to shout “Integrity!” by using her male name or pronoun, which clearly goes against that person’s wishes. It is an act of respect, even if we disagree, to let the person determine what they want to be called. If we can’t grant them that, it’s going to be next to impossible to establish any sort of relationship with them.
The exception is that, as a counselor, I defer to a parent’s preference for their teenager’s name and gender pronoun. Even here I talk with the parent about the benefits and drawbacks of what they want and what their teenager wants if the goal is to establish a sustained, meaningful relationship with their child.
Also, we can avoid gossip about Sara and her family. Gossip fuels the shame that drives people away from the church; gossip prevents whole families from receiving support.
Chapters in Redemption
In some church structures, the person’s spiritual life is under the care of those tasked with leading a local congregation. In this case, we have to trust church leadership to do the hard work of shepherding everyone who accepts Christ as Lord and Savior. We trust, too, that God is working in the lives of our leaders to guide them in wisdom and discernment. We trust that meaningful conversations are taking place, and we can add our prayers for any follower of Christ.
In other church settings, it might be us as laypeople who are called into a redemptive relationship with the transgender person. After all, Christians are to facilitate communities in which we are all challenged to grow as disciples of Christ. We can be sensitive, though, not to treat as synonymous management of gender dysphoria and faithfulness. Some may live a gender identity that reflects their biological sex, depending on their discomfort. Others may benefit from space to find ways to identify with aspects of the opposite sex, as a way to manage extreme discomfort. And of course, no matter the level of discomfort someone with gender dysphoria experiences (or the degree to which someone identifies with the opposite sex), the church will always encourage a personal relationship with Christ and faithfulness to grow in Christlikeness.
Certainly we can extend to a transgender person the grace and mercy we so readily count on in our own lives. We can remind ourselves that the book of redemption in a person's life has many chapters. You may be witness to an early chapter of this person's life or a later chapter. But Christians believe that God holds that person and each and every chapter in his hands, until that person arrives at their true end—when gender and soul are made well in the presence of God.
1 in 4 Pastors Have Struggled with Mental Illness, Finds LifeWay and Focus on the Family
Family ministry has LifeWay Research examine how well (or not well) churches address mental health.
Sarah Eekhoff Zylstra
[ posted 9/22/2014 ]
[Updated with Ed Stetzer quotes]
Your pastor is just as likely to experience mental illness as any other American, according to a LifeWay Research survey commissioned by Focus on the Family.
Nearly 1 in 4 pastors (23 percent) acknowledge they have “personally struggled with mental illness,” and 12 percent of those pastors said the illness had been diagnosed, according to the poll (infographics below). One in four U.S. adults experience mental illness in a given year, according to the National Alliance on Mental Illness.
“Here’s what we know from observation: If you reveal your struggle with mental illness as a pastor, it’s going to limit your opportunities,” Ed Stetzer, executive director of LifeWay Research, told CT. “What happens is pastors who are struggling with mental illness tend not to say it until they are already successful. So Perry Noble, running a church of 30,000 plus, just last year says ‘I have severe depression.’”
“We have to break the stigma that causes people to say that people with mental illness are just of no value,” he added. “These high-profile suicides made it okay to talk about, but I think Christians have been slower than the population at large to recognize what mental illness is, let alone what they should do."
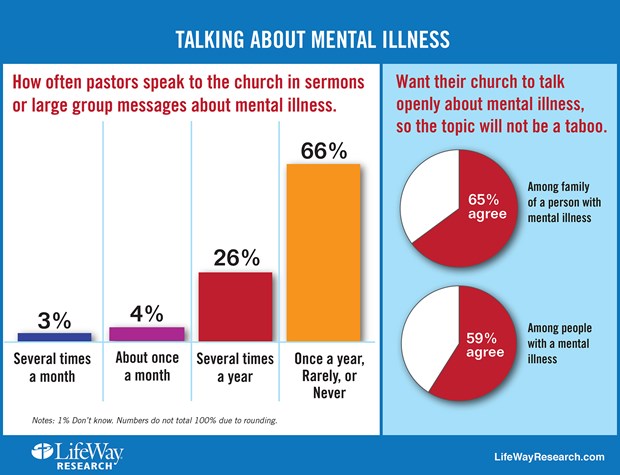
The majority of pastors (66 percent) still rarely or never talk about mental illness in sermons or before large groups, the survey found. About one-fourth of pastors bring up mental illness several times a year, and 7 percent say they tackle it once a month or more.
Image: LifeWay Research
Struggling laypeople wish their churches dealt with the issue more; 59 percent of respondents with a mental illness want their church to talk more openly about it, as do 65 percent of their family members.
“Our research found people who suffer from mental illness often turn to pastors for help,” Stetzer noted in a news release. “But pastors need more guidance and preparation for dealing with mental health crises. They often don’t have a plan to help individuals or families affected by mental illness, and miss opportunities to be the church.”
Other “key disconnects” uncovered by the study:
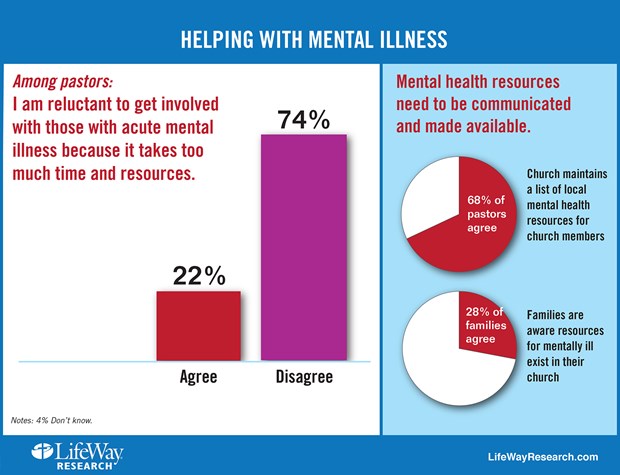
Two-thirds of pastors (68 percent) say their church maintains a list of local mental health resources for church members. But few families (28 percent) are aware those resources exist.
Only a quarter of churches (27 percent) have a plan to assist families affected by mental illness, according to pastors. And only 21 percent of family members are aware of a plan in their church.
Few churches (14 percent) have a counselor skilled in mental illness on staff, or train leaders how to recognize mental illness (13 percent), according to pastors.
The disconnect isn’t because of a lack of compassion. Most pastors (74 percent) say they aren’t reluctant to get involved with those with acute mental illnesses, and nearly 60 percent have provided counseling to people who were later diagnosed.
Image: LifeWay Research
Instead, pastors can feel overwhelmed at times with how to properly respond to the mental health needs of members of their congregation; 22 percent said they were reluctant to do more because it took “too much time.”
“Pastors are trained for spiritual struggle. They’re not trained for mental illness,” Stetzer told CT. “And so, what they will often do is pass someone off. I don’t think what that 20 percent says is ‘Forget you,’ but ‘I can’t handle this.’”
The silence at church can lead to a reluctance to share, Atlanta-based psychiatrist Michael Lyles told LifeWay. “The vast majority of [my evangelical Christian patients] have not told anybody in their church what they were going through, including their pastors, including small group leaders, everybody,” he said in the release.
In fact, 10 percent of the 200 respondents with mental illness said they have switched churches after a church’s poor response to them, and another 13 percent stopped going altogether or couldn’t find a church.
But more than half of regular churchgoers with mental illness said they stayed where they were, and half also said that their church has been supportive. One way churches can be supportive, Stetzer suggested to CT, is regular meetings between pastoral staff and the person suffering from mental illness, even as the individual continues to receive consistent medical treatment.
“The Bible is filled with people who struggled with suicide, or were majorly depressed or bi-polar,” said Focus on the Family pyschologist Jared Pingleton in the LifeWay release. “David was totally bi-polar. Elijah probably was as well. They are not remembered for those things. They are remembered for their faith.”
Researchers focused on three groups:
They surveyed 1,000 senior Protestant pastors about how their churches approaches mental illness. Researchers then surveyed 355 Protestant Americans diagnosed with an acute mental illness—either moderate or severe depression, bipolar, or schizophrenia. Among them were 200 church-goers.
A third survey polled 207 Protestant family members of people with acute mental illness.
Researchers also conducted in-depth interview with 15 experts on spirituality and mental illness.
NASHVILLE, Tenn. – One in four Americans suffers from some kind of mental illness in any given year, according to the National Alliance on Mental Illness. Many look to their church for spiritual guidance in times of distress.But they're unlikely to find much help on Sunday mornings.
Most Protestant senior pastors (66 percent) seldom speak to their congregation about mental illness.
That includes almost half (49 percent) who rarely (39 percent) or never (10 percent), speak about mental illness. About 1in 6 pastors (16 percent) speak about mental illness once a year. And about quarter of pastors (22 percent) are reluctant to help those who suffer from acute mental illness because it takes too much time.
Those are among the findings of a recent study of faith and mental illness by Nashville-based LifeWay Research. The study, co-sponsored by Focus on the Family, was designed to help churches better assist those affected by mental illness.
Researchers looked at three groups for the study.
They surveyed 1,000 senior Protestant pastors about how their churches approaches mental illness. Researchers then surveyed 355 Protestant Americans diagnosed with an acute mental illness—either moderate or severe depression, bipolar, or schizophrenia. Among them were 200 church-goers.
A third survey polled 207 Protestant family members of people with acute mental illness.
Researchers also conducted in-depth interview with 15 experts on spirituality and mental illness.
The study found pastors and churches want to help those who experience mental illness. But those good intentions don’t always lead to action.
"Our research found people who suffer from mental illness often turn to pastors for help," said Ed Stetzer, executive director of LifeWay Research.
"But pastors need more guidance and preparation for dealing with mental health crises. They often don’t have a plan to help individuals or families affected by mental illness, and miss opportunities to be the church."
A summary of findings includes a number of what researchers call ‘key disconnects’ including:
Only a quarter of churches (27 percent) have a plan to assist families affected by mental illness according to pastors.And only 21 percent of family members are aware of a plan in their church. Few churches (14 percent) have a counselor skilled in mental illness on staff, or train leaders how to recognize mental illness (13 percent) according to pastors. Two-thirds of pastors (68 percent) say their church maintains a list of local mental health resources for church members. But few families (28 percent) are aware those resources exist. Family members (65 percent) and those with mental illness (59 percent) want their church to talk openly about mental illness, so the topic will not be a taboo. But 66 percent of pastors speak to their church once a year or less on the subject.
That silence can leave people feeling ashamed about mental illness, said Jared Pingleton, director of counseling services at Focus on the Family. Those with mental illness can feel left out, as if the church doesn’t care. Or worse, they can feel mental illness is a sign of spiritual failure.
"We can talk about diabetes and Aunt Mable’s lumbago in church—those are seen as medical conditions,” he said. “But mental illness--that’s somehow seen as a lack of faith."
Most pastors say they know people who have been diagnosed with mental illness. Nearly 6 in 10 (59 percent) have counseled people who were later diagnosed.
And pastors themselves aren’t immune from mental illness. About a quarter of pastors (23 percent), say they’ve experienced some kind of mental illness, while 12 percent say they received a diagnosis for a mental health condition.
But those pastors are often reluctant to share their struggles, said Chuck Hannaford, a clinical psychologist and president of HeartLife Professional Soul-Care in Germantown, Tennessee. He was one of the experts interviewed for the project.
Hannaford counsels pastors in his practice and said many – if they have a mental illness like depression or anxiety—won’t share that information with the congregation.
He doesn't think pastors should share all the details of their diagnosis. But they could acknowledge they struggle with mental illness.
"You know it’s a shame that we can’t be more open about it,” he told researchers. “But what I’m talking about is just an openness from the pulpit that people struggle with these issues and it’s not an easy answer."
Those with mental illness can also be hesitant to share their diagnosis at church. Michael Lyles, an Atlanta-based psychiatrist, says more than half his patients come from an evangelical Christian background.
"The vast majority of them have not told anybody in their church what they were going through, including their pastors, including small group leaders, everybody," Lyle said.
Stetzer said what appears to be missing in most church responses is "an open forum for discussion and intervention that could help remove the stigma associated with mental illness."
"Churches talk openly about cancer, diabetes, heart attacks and other health conditions – they should do the same for mental illness, in order to reduce the sense of stigma," Stetzer said.
Researchers asked those with mental illness about their experience in church.
A few – (10 percent)—say they’ve changed churches because of how a particular church responded to their mental illness. Another 13 percent ether stopped attending church (8 percent) or could not find a church (5 percent). More than a third, 37 percent, answered, “don’t know,” when asked how their church’s reaction to their illness affected them. Among regular churchgoers with mental illness, about half (52 percent) say they have stayed at the same church. Fifteen percent changed churches, while 8 percent stopped going to church, and 26 percent said, “Don’t know.” Over half, 53 percent, say their church has been supportive. About thirteen percent say their church was not supportive. A third (33 percent) answered, “don’t know” when asked if their church was supportive.
LifeWay Research also asked open-ended questions about how mental illness has affected people’s faith. Those without support from the church said they struggled.
“My faith has gone to pot and I have so little trust in others,” one respondent told researchers.
“I have no help from anyone,” said another respondent.
But others found support when they told their church about their mental illness.
“Several people at my church (including my pastor) have confided that they too suffer from mental illness,” said one respondent. “Reminding me that God will get me through and to take my meds,” said another.
Mental illness, like other chronic conditions, can feel overwhelming at times, said Pingleton. Patients can feel as if their diagnosis defines their life. But that’s not how the Bible sees those with mental illness, he said.
He pointed out that many biblical characters suffered from emotional struggles. And some, were they alive today, would likely be diagnosed with mental illness.
“The Bible is filled with people who struggled with suicide, or were majorly depressed or bi-polar, he said. “David was totally bi-polar. Elijah probably was as well. They are not remembered for those things. They are remembered for their faith.”
LifeWay Research’s study was featured in a two-day radio broadcast from Focus on the Family on September 18 and 19. The study, along with a guide for pastors on how to assist those with mental illness and other downloadable resources, are posted at ThrivingPastor.com/MentalHealth.
LifeWay Research also looked at how churches view the use of medication to treat mental illness, about mental and spiritual formation, among other topics. Those findings will be released later this fall.
Methodology: LifeWay Research conducted 1,000 telephone surveys of Protestant pastors May 7-31, 2014. Responses were weighted to reflect the size and geographic distribution of Protestant churches. The sample provides 95% confidence that the sampling error does not exceed +3.1%. Margins of error are higher in sub-groups.
LifeWay Research conducted 355 online surveys July 4-24, 2014among Protestant adults who suffer from moderate depression, severe depression, bipolar, or schizophrenia. The completed sample includes 200 who have attended worship services at a Christian church once a month or more as an adult.
LifeWay Research conducted 207 online surveys July 4-20, 2014 among Protestant adults who attend religious services at a Christian church on religious holidays or more often and have immediate family members in their household suffering from moderate depression, severe depression, bipolar, or schizophrenia.
Posted by: Dr. Dan L. Boen AT 01:18 pm
| Permalink
| Email
It's as accurate as current methods, but can also confirm recovery, researchers contend
URL of this page: http://www.nlm.nih.gov/medlineplus/news/fullstory_148403.html (*this news item will not be available after 12/15/2014)
Tuesday, September 16, 2014
TUESDAY, Sept. 16, 2014 (HealthDay News) -- A new blood test is the first objective scientific way to diagnose major depression in adults, a new study claims.
The test measures the levels of nine genetic indicators (known as "RNA markers") in the blood. The blood test could also determine who will respond to cognitive behavioral therapy, one of the most common and effective treatments for depression, and could show whether the therapy worked, Northwestern University researchers report.
Depression affects nearly 7 percent of U.S. adults each year, but the delay between the start of symptoms and diagnosis can range from two months to 40 months, the study authors pointed out.
"The longer this delay is, the harder it is on the patient, their family and environment," said lead researcher Eva Redei, a professor in psychiatry and behavioral sciences and physiology at Northwestern's Feinberg School of Medicine in Chicago.
"Additionally, if a patient is not able or willing to communicate with the doctor, the diagnosis is difficult to make," she said. "If the blood test is positive, that would alert the doctor."
The study, published online Sept. 16 in Translational Psychiatry, with funding from the U.S. National Institute of Mental Health and the Davee Foundation, established the test's effectiveness with 32 adults who were diagnosed as depressed and 32 nondepressed adults. All of the study participants were between 21 and 79 years old.
The test works by measuring the blood concentration of the RNA markers. A cell's RNA molecules are what interpret its genetic code and then carry out those instructions from DNA. After blood is drawn, the RNA is isolated, measured and compared to RNA levels expected in a nondepressed person's blood.
Redei's team administered the blood test to all 64 participants in the study. Then, after 18 weeks of face-to-face or phone therapy for those participants with depression, the test was repeated on 22 of them.
Among the depressed participants who recovered with therapy, the researchers identified differences in their RNA markers before and after the therapy. Meanwhile, the concentration of RNA markers of patients who remained depressed still differed from the original results of the nondepressed patients.
Three of the RNA markers in the adults who recovered remained a little different from those who were never depressed, indicating the possibility that these markers might show a susceptibility to depression, the authors noted.
Additionally, if the levels of five specific RNA markers line up together, that suggests that the patient will probably respond well to cognitive behavioral therapy, Redei said. "This is the first time that we can predict a response to psychotherapy," she added.
The blood test's accuracy in diagnosing depression is similar to those of standard psychiatric diagnostic interviews, which are about 72 percent to 80 percent effective, she said.
The findings were welcomed by one mental health expert.
"The mental health profession has, for decades, been seeking an objective measure for detecting major psychiatric disorders," said Dr. Glen Elliott, chief psychiatrist and medical director of the Children's Health Council in Palo Alto, Calif. "That the authors seem to have found a measure in such a small sample that appears to be sensitive to a specific treatment -- and a psychological intervention at that -- is striking if it holds up."
However, he noted that the small number of study participants means that it is too soon to know the significance of the findings or what the drawbacks of the test could be.
"It is too early to tell how a test of this nature -- even if proven reliable, sensitive and specific -- would be best used in a clinical setting," Elliott said. But he said the findings fit into the larger effort to personalize diagnoses and treatments based on biological data from patients.
"It is an exciting possibility that could, in theory, greatly enhance treatment efficacy and efficiency," Elliott said. "However, especially in psychiatry, we are still a long way from having a reliable product that will accomplish those goals."
The new blood test is not yet available because additional studies with large groups of people must first confirm its accuracy and effectiveness before it can be considered by the U.S. Food and Drug Administration for approval.
Depending on funding, that could take several years, Redei said. If approved, the blood test's costs would be "in the range of other specialty tests," she said.
SOURCES: Eva Redei, Ph.D., David Lawrence Stein Research Professor of Psychiatric Diseases Affecting Children and Adolescents, Asher Center for the Study and Treatment of Depressive Disorders, Northwestern University Feinberg School of Medicine, Chicago; Glen Elliott, Ph.D., M.D., chief psychiatrist and medical director, the Children's Health Council, emeritus professor of clinical psychiatry, University of California, San Francisco, and professor of clinical psychiatry, Stanford School of Medicine, Calif.; Sept. 16, 2014, Translational Psychiatry, online
HealthDay
Copyright (c) 2014 HealthDay. All rights reserved.
At many weddings these days, whether on picturesque hillsides or at funky warehouses or in swanky ballrooms, newly minted husbands and wives proudly declare to friends and family, “I married my best friend.”
If you attended a wedding this summer, you likely heard the phrase, now so standard in romantic rhetoric that we forget it’s not part of the traditional ceremony. “I married my best friend” appears in vows, program dedications, toasts, and other aww-inducing moments (not to mention the cards, frames, cufflinks, wine glasses, and other Etsy-inspired wares that attend modern weddings).
The sentiment, repeated in Facebook posts on anniversaries, is shorthand for the special relationship with someone we are comfortable with, who listens, loves, and encourages. From secular folks to Christians who firmly believe that God sent them the one, nearly all the married people I know are “so blessed” (or “lucky”) to get to spend their lives wedded to their best friends.
Even if couples don’t announce that they’re marrying their best friend, many newlyweds live out this philosophy, dropping out of the friend-making game once they have a ring on their finger. Sociologists find that these days, we typically form our most meaningful friendships prior to age 28. Not coincidentally, that’s also the average age we get married.
Marrying your best friend is enough of a cultural expectation that if I admit I didn’t, people might pity me. But here’s the secret: I’m actually the lucky one. I have a husband who isn’t my best friend. And I have a best friend whom I’m not married to. They play different roles in my life, and I need them both.
One Person Can’t Meet All Your Needs
For Christians, marriage is a relationship set apart, wherein we assume the cares and concerns of our spouse (1 Cor. 7:32–35; Eph. 5:22–33) in a way that supersedes any other friendship. Of course married people find their most significant relationship in their husband or wife—but that doesn’t equate to being BFFs.
I worry that the saying “I married my best friend” conflates the two types of relationships, distorting our views of both.
My marriage remains my priority... But without my friends, my relationship with my husband—and with God—would suffer.
Researchers have already noticed the trend: People increasingly expect their husbands or wives to meet all their social and emotional needs. The phrase implies that, since married people have each other, they don’t have best friends anymore and don’t need them. And it exaggerates the risks young couples already face: setting up unhealthy expectations, looking to each other as the sole source of fulfillment. It also relegates best friends to the realm of singleness.
Making friends in your late 20s and beyond is a whole different game. Not only are there fewer opportunities to meet people, there are also fewer people to meet, since married folks tend to pull themselves off the friendship market. Plenty of young couples dedicate more time to catching up on their Netflix queue than seeing their neighbors, coworkers, and old buddies. My husband and I have been guilty, and so have plenty of our friends. They update Facebook about spending yet another weekend in, joking about becoming “a boring old married couple.”
And yet friends can actually support—not detract from—our marriages. Psychology journalist Carlin Flora writes in her book Friendfluence:
Putting your best self forward for new friends allows you to shine and to see your partner through new eyes as she shines, too. Maintaining older mutual friendships also strengthens the bond between long-term partners: Having people around who think of the two of you as a unit, who admire your relationship, and who expect you to stay together can sustain you through times of doubt or distance.
When I got married, I knew I didn’t want us to become one of those couples who stopped making friends or fell out of touch. Maybe it’s because I knew I couldn’t rely on my husband, who is in the Army, to always be there to meet my needs. Or maybe it’s because I have really incredible friends, whom I’d much rather see Twilight with or ask fashion advice from than my spouse.
Don’t get me wrong: My marriage remains my priority, the place where God has done the most to reveal the gospel to me. But without my friends, my relationship with my husband—and with God—would suffer. I gain much from being around others and receiving their perspectives and their prayers. Time spent with friends also keeps me from idolizing my husband as “my everything,” a habit many married people struggle to resist.
Making Friendship a Priority
I want to intentionally be open to the multiple relationships God will use to work in my life and the many opportunities I may have in others’. But those kinds of relationships don’t happen by accident. Here’s where friendship is like marriage: It takes work.
On her sitcom The Mindy Project, Mindy Kaling declares, “A best friend isn’t a person. It’s a tier.” I’m in her camp. I have a best friend from growing up, a best friend from college, and others from my early 20s. It’d be easy for these relationships to fizzle out, so I make it a priority to visit, even when it requires sacrifice, and to regularly text, call, and write in between.
We moved around a lot when I was growing up. Always the new girl in school, I think back to a note my mom placed in my lunchbox: “To make a friend, you have to be a friend.” Decades later, I’ve found it still takes initiative and effort to sustain friendships. If we look to Jesus as an example, he selected friends to invest in. He had a best friend (John) and a best friend tier (the disciples). He says to them in John 15:12–15 (ESV):
This is my commandment, that you love one another as I have loved you. Greater love has no one than this, that someone lay down his life for his friends. You are my friends if you do what I command you. No longer do I call you servants, for the servant does not know what his master is doing; but I have called you friends, for all that I have heard from my Father I have made known to you.
Verse after Bible verse speaks of the “sweetness” (Prov. 27:9, ESV) and value of faithful friends. God wouldn’t have us give up these relationships for marriage, but continue to sharpen (Prov. 27:17) and grow one another in this special context.
We regularly talk about upholding and enhancing marriage and family life for their gospel witness, as we should. I’d like us to start doing the same with friendship. We need friends not only for our health, careers, and happiness, but more importantly, for the way they witness to our siblinghood in Christ. And from the meaningful ties of friendship often come opportunities to introduce others to Jesus, the one who calls us his friends in the first place (John 15:15).
I didn’t marry my best friend. Instead, I married my husband, with all my best friends beside me to celebrate. It was the happiest day of my life. I got—and still get—to have both.
Kate Shellnutt is associate editor of Her.meneutics, CT’s women’s site.
For an article about ministry and neuroscience, it seems only right to begin with Scripture. So we start with one of the great neurological texts of the Bible: "David put his hand in his bag, and took thence a stone, and slang it, and smote the Philistine in his forehead, that the stone sunk into his forehead; and he fell upon his face to the earth" (1 Sam. 17:49, KJV).
Neuroscience has gained so much attention recently that it can seem like we're the first humans to discover a connection between the physical brain and spiritual development. But way back in Bible times, before EEGs and HMOs, people had noticed that putting a rock through someone's skull tends to inhibit their thinking.
For those of us in church leadership, information about "the neuroscience of everything" is everywhere. How much do we need to know about it? What new light does it shed on human change processes that those of us in the "transformation business" need to know? Does it cast doubt on the Christian view of persons as spiritual beings who are not merely physical?
Why is Neuroscience Exploding?
Neuroscience studies the nervous system in general and the brain in particular. Neurobiology looks at the chemistry of cells and their interactions; cognitive neuroscience looks at how the brain supports or interacts with psychological processes; something called computational neuroscience builds computer models to test theories.
Most of our behavior-typing, tying a shoe, or driving-is governed by habits imprinted on our brains. So is discipleship.
Because the mind can be directed to any topic, there can be a "neuroscience" of almost any topic. Neurotheology looks at the brain as we believe, think, and pray about God. Researcher Andrew Newberg has shown the brain-altering power of such practices as prayer by looking at changes in the brain-state of nuns engaged in the practice for over 15 years as well as Pentecostals praying in tongues. It turns out that intense practice of prayer means their brains are much more impacted by their prayer than inexperienced or casual pray-ers. To find out who the true prayer-warriors in your church are, you could hook everybody up to electrodes, but it might be a little embarrassing. Paul Bloom pointed out that we shouldn't be surprised by this; the surprising thing would be if people experience a profound state without their brains being affected.
Brain studies made steady progress through the twentieth century; my own original doctoral advisor at Fuller Seminary was Lee Travis, who pioneered the use of the electroencephalogram at the University of Iowa in the 1930s. But for a long time, no one could actually look inside a working brain to watch it in operation.
That changed in the 1990s with functional Magnetic Resonance Imaging (fMRI), which allows researchers to track the flow of oxygen-rich blood (a proxy for neuron activity) in real time. Now it became possible to find out what part of the brain is involved in any given sequence of conscious activity, and how brain functions of liberals versus conservatives or religious versus non-religious people may differ from each other. It also became possible to find out if that guy in the second row whose eyes are closed when you're preaching really does have something going on in his brain during the sermon.
Why I'm Thankful for Neuroscience
"All truth is God's truth," Augustine said, and a deep part of what it means to "exercise dominion" is to learn all we can about what God has created. And there is very little God created that is more fascinating or more relevant to our well-being than our brains.
Neuroscience has immense potential to relieve human suffering. Already neuroscientists have found ways to alleviate symptoms of Parkinsons and create cochlear implants. Our church had a baptism service recently and several of those being baptized were young adults who suffer from cognitive challenges. In each case their parents were in tears. For those of us doing ministry to be aware of advances in brain science is part of caring for those in our congregation.
Research into the teenage brain made clear that the human brain isn't really fully developed until people are well into their twenties. Previously it was thought that the teenage brain was just "an adult brain with fewer miles on it." It turns out that the frontal lobes, which are associated with choosing and decision-making as well as with impulse-control and emotional management, are not fully connected—they lack the myelin coating that allows efficient communication between one part of the brain and another.
Christians have brains and neurons that are as fallible as atheist neurons and new age neurons.
This helps explains the ancient mantra of parents and student ministry leaders everywhere: "What were you thinking?" Churches can help parents of teenagers understand why a practice as simple as insisting their teenage children get a good night's sleep is so necessary. They can also help parents set expectations for their teenagers' emotional lives at an appropriate level. They can also remind church leaders who are doing talks for teenagers to keep them short!
Neuroscience can also teach us compassion. For too long people who suffered from emotional or mental illness have been stigmatized. Churches—which should have been the safest places to offer healing and care—were sometimes among the most judgmental communities because it was assumed that if people simply got their spiritual lives together, their emotions should be fine.
Rick and Kay Warren noted after the death of their son: "Any other organ in my body can get broken and there's no shame, no stigma to it. My liver stops working, my heart stops working, my lungs stop working. Well, I'll just say, 'Hey, I've got diabetes, or a defective pancreas or whatever,' but if my brain is broken, I'm supposed to feel shame. And so a lot of people who should get help don't."
Pastors can offer great help to their congregation when we simply acknowledge the reality that followers of Jesus do not get a free pass from mental health problems. Christians have brains and neurons that are as fallible as atheist neurons and New Age neurons.
Beyond that, I'm thankful for neuroscience because it is helping us understand better how our bodies work, and that enables us better to "offer our bodies a living sacrifice to God." Knees that spend long hours in prayer change their shape. So do brains.
The Limits of Neuroscience
One of the reasons it's important for pastors to be conversant with the topic is that neuroscience is being accorded enormous authority in our day—not always for good reasons. I joke with a neuroresearcher friend of mine (who helped a lot with this article but wants to remain anonymous) that the easiest way to get an article published today is to pick any human behavior and …
Show which parts of the brain are most active when thinking about that topic;
Explain why evolutionary psychology has shown that behavior is important to our survival;
Give four common-sense tips for handling that behavior better—none of which has anything to do with #1 or #2.
Precisely because neuroscience has so much prestige, those of us who teach at churches need to be aware of its limitations as well as its findings. It's one thing to say that our brain chemistry or genetic predisposition may affect our attitudes or beliefs or behaviors. It's another thing to say we are nothing but our brain chemistry.
Sometimes writers make claims in popular literature that would never make it into a peer-reviewed academic journal. One example is a recent book, We Are Our Brains, which makes the claim that there is no such thing as free will, that our brains predetermine everything including our moral character and our religious leanings, so there is no good reason to believe God exists either.
Because neuroscience has so much prestige, we church leaders need to be aware of its limitations as well as its findings.
People may be under the impression that "science" has proven this. This is sometimes called "nothing buttery"; the idea that we are "nothing but" our physical selves.
Yet let's be clear: we are not just our brains.
No one has ever seen a thought, or an idea, or a choice. A neuron firing is not the same thing as a thought, even though they may coincide. A brain is a thing, a human being is a person.
God doesn't have a brain, Dallas Willard used to say, and he's never missed it at all. (Dallas actually used to say that's why for God every decision is a "no-brainer," but I will not repeat that because it's too much of a groaner, even for Dallas.)
Neuroscience can help us understand moral and spiritual development. It shows the importance of genetic predispositions in areas of character and attitudes—from political orientation to sexuality. But it has not shown that personal responsibility or dependence on God are irrelevant. It does not replace the pastor or trump the Bible.
The Neuroscience of Sin And Habits
Neuroscience has shown us in concrete ways a reality of human existence that is crucial for disciples to understand in our struggle with sin. That reality is this: mostly our behavior does not consist of a series of conscious choices. Mostly, our behavior is governed by habit. Most of the time, a change of behavior requires the acquisition of new habits. Willpower and conscious decision have very little power over what we do.
A habit is a relatively permanent pattern of behavior that allows you to navigate life. The capacity for habitual behavior is indispensible. When you first learn how to type or tie a shoe or drive a car, it's hard work. So many little steps to remember. But after you learn, it becomes habitual. That means it is quite literally "in your body" (or "muscle memory"). At the level of your neural pathways. Neurologists call this process where the brain converts a sequence of actions into routine activity "chunking."
Chunking turns out to be one of the most important dynamics in terms of sin and discipleship. Following Jesus is, to a large degree, allowing the Holy Spirit to "re-chunk" my life. This is a physical description of Paul's command to the Romans: " … but be transformed by the renewing of your mind."
Habits are enormously freeing. They are what allows my body to be driving my car while my mind is planning next week's sermon.
But sin gets into our habits. This is the tragedy of fallen human nature. Self-serving words just come out of my mouth; jealousy comes unbidden when I meet someone who leads a larger church or preaches better; chronic ingratitude bubbles up time and again; I cater to someone I perceive to be attractive or important.
Neuroscience research gives us a clearer picture (and deeper fear) of what might be called the "stickiness" of sin. It is helping us to understand more precisely, or at least more biologically, exactly what Paul meant when he talked about sin being "in our members." He was talking about human beings as embodied creatures—sin is in the habitual patterns that govern what our hands do and where our eyes look and words our mouths say. Habits are in our neural pathways. And sin gets in our habits. So sin gets in our neurons.
Like so much else, our neurons are fallen, and can't get up. They need redemption.
The Neuroscience of Discipleship
You can override a habit by willpower for a moment or two. Reach for the Bible. Worship. Pray. Sing. You feel at peace with God for a moment. But then the sinful habit reemerges.
Habits eat willpower for breakfast.
When Paul says there is nothing good in our "sinful nature," he is not talking about a good ghost inside you fighting it out with a bad ghost inside you. Paul is a brilliant student of human life who knows that evil, deceit, arrogance, greed, envy, and racism have become "second nature" to us all.
Sanctification is, among other things, the process by which God uses various means of grace to re-program our neural pathways. This is why Thomas Aquinas devoted over 70 pages of the Summa Theologica to the cultivation of holy habits.
It's why 12-step groups appeal, not to willpower, but to acquiring new habits through which we can receive power from God to do what willpower never could.
Neuroscience has helped to show the error of any "spirituality" that divorces our "spiritual life" from our bodies. For example, it has been shown that the brains of healthy people instructed to think about a sad event actually look a lot like the brains of depressed people.
"Spiritual growth" is not something that happens separate from our bodies and brains; it always includes changes within our bodies. Paul wrote, "I beat my body to make it my slave"—words that sound foreign to us, but in fact describe people who seek to master playing the cello or running a marathon. I seek to make the habits and appetites of my body serve my highest values, rather than me becoming a slave to my habits and appetites. What makes such growth spiritual is when it is done through the power and under the guidance of the Holy Spirit. Paul's language remains unimprovable: We offer our bodies as living sacrifices so that our minds can be renewed.
One of the great needs in churches is for pastors and congregations to experiment with discipleship pathways that address the particular context that we face. Pornography (and misguided sexuality in general) has always rewired the brain. But now porn is so incredibly accessible that men and women can be exposed to it any time they want for as long as they want as privately as they want. Each time that connection between explicit images and sexual gratification is established, the neural pathway between the two grows deeper—like tires making ever-deepening ruts in a road.
Simply hearing that sexual sin is bad, or hearing correct theological information, does not rewire those pathways. What is required is a new set of habits, which will surely include confession and repentance and fellowship and accountability and the reading of Scripture, through which God can create new and deeper pathways that become the new "second nature," the "new creation."
At our church not long ago, one of our members spoke openly about many years of shame around sexual addiction. His courageous openness stilled the congregation, and it led to the formation of a recovery ministry that is one of the most vibrant in our church.
The Neuroscience of Virtue
Kent Dunnington has written a wonderfully helpful book, Addiction and Virtue. He notes that many federal health institutes and professional organizations assume addiction is a "brain disease" purely "because the abuse of drugs leads to changes in the structure and function of the brain." However, playing the cello and studying for a London taxi license and memorizing the Old Testament also lead to changes in the structure and function of the brain. Shall we call them diseases, too?
Dunnington says that addiction is neither simply a physical disease nor a weakness of the will; that to understand it correctly, we need to resurrect an old spiritual category: habit. We have habits because we are embodied creatures; most of our behaviors are not under our conscious control. That's a great gift from God—if we had to concentrate on brushing our teeth or tying our shoes every time we did that, life would be impossible.
But sin has gotten into our habits, into our bodies, including our neurons.
Partly, we may be pre-disposed to this.
For example, people with a version of the Monoamine oxidase A (MOA) gene that creates less of the enzyme tend to have more troubles with anger and impulse control. (If you have that version of MOA, you're feeling a little testy right now.) This means that when Paul says "In your anger, do not sin," some people are predisposed to struggle with this more than others.
That doesn't mean that such people are robots or victims or not responsible for their behavior. It does explain part of why Jesus tells us to "Judge not"; none of us knows the genetic material that any other person is blessed with or battling in any given moment.
This also shows that the people in our churches will not be transformed simply by having more exegetical or theological information poured into them—no matter how correct that information may be. The information has to be embodied, has to become habituated into attitudes, patterns of response, and reflexive action.
The reason that spiritual disciplines are an important part of change is that they honor the physical nature of human life. Information alone doesn't override bad habits. God uses relationships, experiences, and practices to shape and re-shape the character of our lives that gets embedded at the most physical level.
A few decades ago scientists did a series of experiments where monkeys were taught how to pinch food pellets in deep trays. As the monkeys got faster at this practice, the parts of the brain controlling the index finger and thumb actually grew bigger. This and other experiments showed that the brain is not static as had often been thought, but is dynamic, able to change from one shape to another. This is true for human beings as well. The part of violinists' brains that controls their left hand (used for precise fingering movements) will be bigger than the part that controls their right hand.
But wait—there's more. In another study, people were put into one of three groups; one group did nothing; one exercised their pinky finger, a third group spent 15 minutes a day merely thinking about exercising their pinky finger. As expected the exercisers got stronger pinkies. But amazingly—so did the people who merely thought about exercising. Changes in the brain can actually increase physical strength.
No wonder Paul wrote: "Whatever is true, whatever is honorable, whatever is just, whatever is pure, whatever is pleasing, whatever is commendable, if there is anything worthy of praise, think about these things." Every thought we entertain is, in a real sense, doing a tiny bit of brain surgery on us.
Here's a thought worth contemplating: what must Jesus' brain have been like? Imagine having neural circuits honed and trained to trust God, to respond to challenge with peace, or to irritation with love, or to need with confident prayer.
Here's another thought worth contemplating: We have the mind of Christ.
That's worth wrapping your brain around.
John Ortberg is pastor of Menlo Park Presbyterian Church in California.















































































































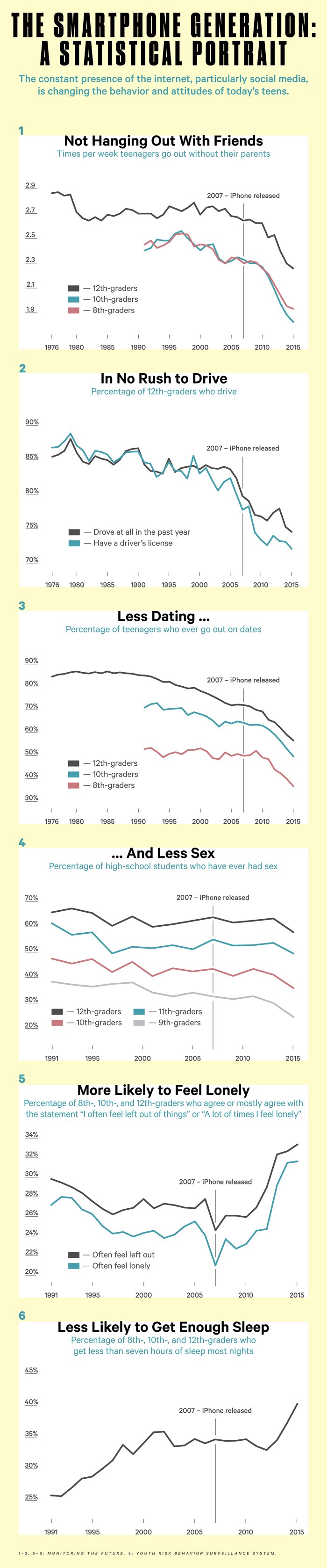




















")